A resurgence in respiratory illness in Manitoba has caused some non-urgent pediatric surgery postponements, health officials say.
Article content
As of Thursday morning, there were 17 patients in the pediatric intensive care unit (PICU) when the baseline capacity is nine, Shared Health said in a statement.
Article content
Shared Health says a “significant” number of the patients were experiencing complex cases that were further complicated by respiratory illness, including infants and young children.
As a result of the pressure on the PICU, approximately 10 staff are being temporarily reassigned to support that unit. While urgent and life-threatening surgeries will continue to happen, some non-urgent procedures could be postponed. Shared Health said families of affected patients will be contacted.
Shared Health said a mix of respiratory illnesses are circulating in the community and have a more profound effect on young children.
Article content
In the children’s emergency department, patient volumes remain “relatively” stable, Shared Health said.
“However, the number of pediatric patients visiting the ED with influenza-like symptoms has increased in the past two weeks, from a low of 22 on March 18 to 47 yesterday,” a news release reads.
There were 51 patients in the neonatal ICU (NICU) on Thursday morning. The normal capacity is 50.
Health officials are reminding parents that their children should not interact with people experiencing cold-like symptoms. That also includes people who may not know or acknowledge that they are unwell and want to hold or kiss their child.
Shared Health also reported that wait times in the adult emergency department largely remain unchanged in February. There was a small increase in median waits but an improvement in the 90th percentile times.
Article content
Overall median wait times in Winnipeg hospitals were 2.77 hours in February, which was a three-minute increase from January. Ninetieth percentile wait times improved by 21 minutes to 7.17 hours across Winnipeg.
Patient volumes increased in February to a daily average of 750, which was up from 730.4 in January with the median length of stay for patients in emergency or urgent care being 21.77 hours, which is down from 22.5 hours in January.
12.1% of patients were left without being seen, which is down from 13% in January. At the Health Sciences Centre, the left without being seen rate dropped to 23.4% in February compared to 25% in January.
A new $2.9 million minor treatment clinic at HSC aimed at improving the rate of patients leaving without being seen and addressing more non-urgent illnesses or injuries is slated to open this summer.
rstelter@postmedia.com
To sign up for Ryan’s weekly newsletter GIMME STELTER, click here.
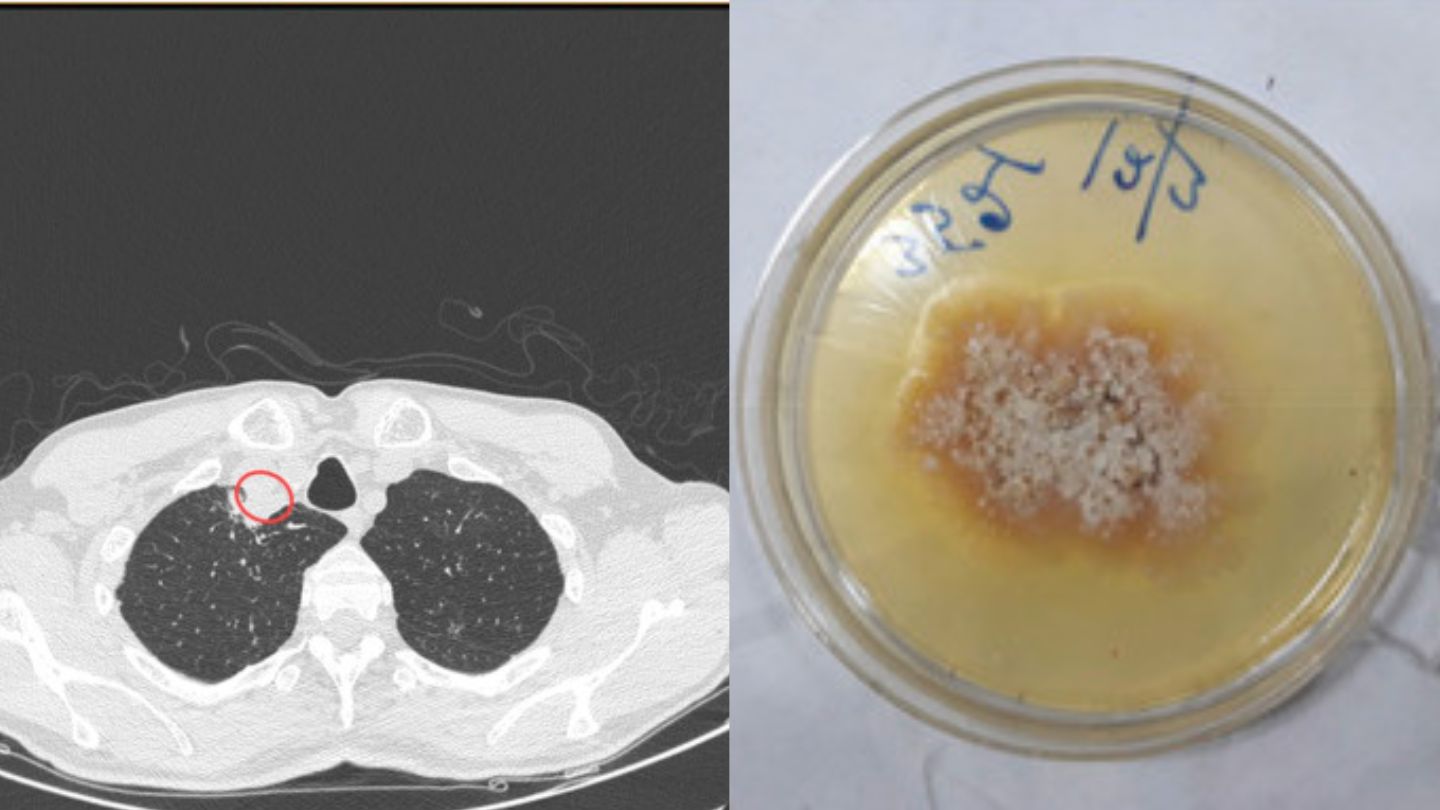
A man in India is the first human known to be infected by a fungus called Chondrostereum purpureum, a pathogen that is most well-known for causing a disease called silver leaf in plants, reports a new study.
The patient, who was 61 at the time of the diagnosis, made a full recovery and has not experienced any recurrence of the infection after two years of follow-up observations. However, this “first of its kind” case study exemplifies the risks that fungal pathogens pose for humans, especially now that climate change and other human activities like rampant urbanization, have opened a “Pandora’s Box for newer fungal diseases” by contributing to their spread, according to the study.
Fungal pathogens are having a pop culture moment because they are the source of a fictional disease depicted in apocalyptic game The Last of Us, which was recently adapted into the acclaimed HBO series of the same name. But these microbes are also a real-life scourge that infect about 150 million people every year, resulting in about 1.7 million deaths.
Though millions of fungal species exist, only a very small fraction of them are able to infect animals, including humans, because our bodies present challenges to these invaders such as high temperatures and sophisticated immune systems.
Soma Dutta and Ujjwayini Ray, doctors at Apollo Multispecialty Hospitals in Kolkata, India, have now added one more fungus to that small list of human invaders with their unprecedented report of a C. purpureum infection. The patient, a plant mycologist, had suffered from cough, fatigue, anorexia, and a throat abscess for months before his hospital visit, and was probably exposed to the fungus as a result of his profession.
When conventional techniques failed to diagnose the disease, the pathogen was sent to a World Health Organization center based in India where it was finally identified using DNA sequencing. The case “highlights the potential of environmental plant fungi to cause disease in humans and stresses the importance of molecular techniques to identify the causative fungal species,” according to their recent study in the journal Medical Mycology Case Reports.
“This is a first of its kind of a case wherein this plant fungus caused disease in a human,” Dutta and Ray said in the study. “This case report demonstrates the crossover of plant pathogens into humans when working in close contact with plant fungi. The cross-kingdom pathogenicity demands much work to be done in order to explore insights of the mechanisms involved, thus leading to possible recommendations to control and contain these infections.”
C. purpureum can infect a variety of different plants with silver leaf disease, an often fatal condition that is named after the color that the pathogen induces on the leaves on the hosts. It is the latest in a growing number of fungal pathogens that have infected humans, which are buoyed on in part by human activities, such as urbanization, travel, and commerce.
Human-driven climate change is also accelerating the spread of infectious diseases, including fungal pathogens, by allowing microbes to adapt to higher temperatures (like those in mammal bodies), expand their range, and interact with new hosts in the aftermath of extreme weather events. And though fungal diseases have maintained a lower profile in epidemiology compared to other pathogens, they may be more dangerous than viruses or bacteria in some contexts.
“While viral and bacterial diseases receive most attention as the potential cause of plagues and pandemics, fungi can arguably pose equal or even greater threats,” according to a 2021 study inPLoS Pathogens. “There are no vaccines available yet for fungal pathogens, the arsenal of antifungal agents is extremely limited, and fungi can live saprotrophically, producing large quantities of infectious spores and do not require host-to-host contact to establish infection. Indeed, fungi seem to be uniquely capable of causing complete host extinction.”
In addition to avoiding the spread of new fungal pathogens that can directly infect humans, researchers also point to the damage these diseases can deal to crops and ecosystems that people depend on. For this reason, Dutta and Ray recommend more research into the nature of these infections and strategies to mitigate their spread.
“Cross-kingdom human pathogens, and their potential plant reservoirs, have important implications for the emergence of infectious diseases,” Dutta and Ray said. “Fungi are also responsible for various infections in plants that cause destruction of millions of plants and crops” and “produce toxins that contaminate food and cause acute toxicity.”
“Over the past several decades multiple new pathogenic fungi have emerged,” they concluded. “A notable emergence of the multidrug resistant fungus Candida auris has spread all over the world and has become a significant threat. The worsening of global warming and other civilization activities opens Pandora's Box for newer fungal diseases.”
The numbers of babies born with syphilis in Canada are rising at a far faster rate than recorded in the United States or Europe, an increase public health experts said is driven by increased methamphetamine use and lack of access to the public health system for Indigenous people.
While syphilis has made a global resurgence over the last five years, Canada is an outlier among wealthy nations in its rate of increase: 13-fold over five years, according to Health Canada. The incidence of babies born with syphilis reached 26 per 100,000 live births in 2021, the most recent year available, up from 2 in 2017, according to the Health Canada data.
That total is on track to increase further in 2022, according to the preliminary government data obtained by Reuters.
Babies with congenital syphilis are at higher risk of low birthweight, bone malformations and sensory difficulties, according to the World Health Organization (WHO).
Syphilis in pregnancy is the second-leading cause of stillbirth worldwide, the WHO said.
Yet congenital syphilis is easily preventable if an infected person gets access to penicillin during their pregnancy.
Among the G7 group of wealthier nations for which data is available, only the United States had a higher incidence of syphilis at birth: 74 per 100,000 live births in 2021, triple the rate in 2017, according to preliminary figures from the U.S. Centers for Disease Control and Prevention (CDC).
Syphilis cases nearly triple in Saskatchewan
There were 2,677 cases of congenital syphilis in the U.S. in 2021 for a population of 332 million, according to preliminary CDC data. Canada had 96 cases for a population of 38 million, according to Health Canada.
People experiencing poverty, homelessness and drug use, and those with inadequate access to the health system, are more likely to contract syphilis through unsafe sex and pass it to their babies, public health researchers said.
“In high-income countries you see it in pockets of disadvantaged populations,” said Teodora Elvira Wi, who works in the WHO’s HIV, Hepatitis and sexually transmitted infection program.
“It’s a marker of inequality. It’s a marker of low-quality prenatal care.”
More on Canada
What sets Canada apart are its Indigenous populations who experience discrimination and often have poor access to health and social services, said Sean Rourke, a scientist with the Li Ka Shing Knowledge Institute at St. Michael’s Hospital in Toronto, who focuses on prevention of sexually transmitted disease.
“It’s just the whole system, and all the things that we’ve done in bad ways not to support Indigenous communities,” he said.
Health Canada told Reuters it has dispatched epidemiologists to help provinces contain the increase in congenital syphilis. Spokesperson Joshua Coke said the federal government is expanding testing and treatment access in Indigenous communities.
Tessa, an Indigenous 28-year-old woman who asked to be identified only by her middle name, said she had a years-long crystal meth addiction and was homeless when she got pregnant in Saskatoon, Saskatchewan.
“I would be walking down the street just crying: ‘Why am I living like this?'” she told Reuters.
She said she received no prenatal care until she went into labor in November, which is when she tested positive for HIV and syphilis during a routine test.
Concerns raised about syphilis in pregnant women
Her daughter was prescribed a 10-day course of antibiotics, administered by IV, and is now healthy, Tessa said. But she still thinks about the difficulties she experienced in accessing prenatal care.
“Having transportation, maybe, and a place to live, and being sober, probably would have helped, big time,” she said.
Susanne Nicolay, nurse lead at Wellness Wheel clinic in Regina, Saskatchewan, which serves Indigenous and vulnerable populations, said providers needed to do more to expand access to health care. “The system always talks about patients that are hard to reach. But I think it’s health providers that are hard to reach,” she said.
'Multiple failures'
A lot needs to go wrong for a baby to be born with syphilis, said Jared Bullard, a Manitoba pediatrician who has been researching babies born with syphilis since 2021 in an ongoing study for the Public Health Agency of Canada.
“It’s pointing at multiple failures along the path,” he said.
In Canada, the rise in babies born with syphilis is concentrated in the three prairie provinces: Manitoba, Saskatchewan and Alberta.
Prairie provinces have higher crystal meth use and remote populations and Indigenous populations who may have trouble accessing health care, Bullard said.
Manitoba recorded the highest rate, with about 371 cases per 100,000 live births in 2021.
Syphilis outbreak in Peterborough
The province said in an emailed statement that it is expanding training for health care providers in addressing sexually transmitted infections, encouraging frequent testing and early treatment. It is digitizing its records of STI infections.
Saskatchewan has launched a public awareness campaign urging people to practice safe sex and get tested, said Dale Hunter, a spokesperson for the provincial health ministry. The province had an incidence of 185 cases of congenital syphilis per 100,00 live births in 2021.
Alberta said women aged 15-29 made up more than half of what it called a “significant increase” in syphilis rates. “The reasons for the increase are not fully known, but it is likely that a variety of factors have contributed to this rise,” Alberta Health Services spokesperson James Wood said.
In preliminary results of a study of 165 infants exposed to syphilis, Bullard and fellow pediatrician Carsten Krueger found at least two-thirds were born to women reporting a history of substance abuse.
About 45% of the women identified as Indigenous and another 40% had no ethnicity recorded. Indigenous people make up about 5% of the Canadian population, according to census data.
About a quarter of the people in the study did not get tested because they got no prenatal care; about one-fifth of those who tested positive did not get treated. Bullard said he has also seen people get treated early in pregnancy and then get re-infected.
Public health researchers and clinicians said the rates of congenital syphilis began increasing before the pandemic and worsened as public health agencies diverted resources to COVID-19 testing and other pandemic-related health measures.
“All of the social circumstances that contributed to this have just gotten worse over the pandemic,” said Ameeta Singh, an infectious diseases specialist with an HIV/STI practice in Edmonton, Alberta.
This month Health Canada approved a syphilis and HIV test that can provide results in less than a minute, allowing providers to begin treatment right away.
Some public health researchers and providers are urging the Canadian government to buy and distribute the tests.
“We probably need a million tests to get out there around the country,” Rourke said. “The solution’s right in front of us.”
Health Canada did not respond when asked about purchasing test kits.
A resurgence in respiratory illness circulating in the province over the past week is contributing to high patient numbers at HSC Children’s pediatric intensive care unit.
There were 17 pediatric patients receiving intensive care this morning. The normal baseline capacity for the pediatric ICU (PICU) is nine. A significant number of these patients were experiencing medically complex cases that were further complicated by respiratory illness, including infants and young children.
A mix of respiratory illnesses are currently circulating in the community. These viruses often have a more profound effect on the health of young children, who are frequently more vulnerable to serious illness.
Patient volumes in the children’s emergency department remain relatively stable. However, the number of pediatric patients visiting the ED with influenza-like symptoms has increased in the past two weeks, from a low of 22 on March 18 to 47 yesterday.
There were 51 patients in the neonatal ICU this morning (NICU). The normal baseline capacity is 50.
In response to the increased pressure on the PICU, approximately 10 staff – including some from pediatric surgical and recovery units – are being temporarily reassigned to support these patients’ care. While all urgent and life-threatening surgeries will continue to be performed, these staffing moves may result in the postponement of some non-urgent procedures. Families of affected patients will be contacted.
In the meantime, we are reminding parents that there are a number of measures they can take to protect their child’s health – the most important of which is ensuring they don’t interact with people experiencing cold-like symptoms. The likelihood of getting sick is directly related to the number of personal interactions a person may have. This includes interactions between young people and individuals who may not know or acknowledge they may be unwell (and who may be looking to hold and kiss the baby).
Parents can also help their children by protecting their own health in a number of ways, such as:
Avoiding close contact with people who are sick;
Regularly washing their hands;
Touching their child’s face with unwashed hands;
Avoiding the sharing of drinks and face towels;
Regularly cleaning high-touch surfaces (door knobs, taps, countertops, etc.) to keep it free of germs;
Sneezing or coughing into one’s elbow instead of hands;
Ensuring they are up to date on their vaccinations; and
Masking when out in large crowds.
Advice for parents on how to treat their sick or injured child, as well as when and where to take them for care, can be viewed at KidCareMB.ca.
Just over a month ago, on Feb. 14, Quebec’s health ministry declared the outbreak over in the province.
The World Health Organization (WHO), however, continues to consider the global situation related to mpox a public health emergency of international concern.
Mpox — which spreads via close contact and tends to cause flu-like symptoms and pus-filled skin lesions — was first declared a global health emergency by the WHO in July 2022.
“The epidemic continues to disproportionately affect men who have sexual relations with other men and the dominant mode of transmission remains direct contact with an infected person during sexual intercourse,” the DRSP said on its website.
Officials said both new infections are in men who contracted the illness elsewhere.
“These are men who have sex with men, who acquired the disease through sexual contact while travelling to countries where local transmission is documented,” the DRSP said.
More on Health
One of the two individuals had received one dose of vaccine, while the other had the two recommended doses. Both presented with typical symptoms without complications. Neither required hospitalization.
Public health says that vaccination with Imvamune reduces the risk of infection and the seriousness of the illness.
“Complete primary vaccination consists of 2 doses at least 28 days apart,” according to public health.
Because of limited quantities of vaccines during the beginning stages of the outbreak in 2022, only one dose was being offered to people who were eligible. That changed at the beginning of October when the second dose was made available.
Public health estimates that 54 per cent of Montreal’s at-risk population has received a first dose of vaccine against mpox, but only around 24 per cent have gotten a second dose.
Public health indicated that analysis of the city’s water suggests there is no local sustained transmission of the disease in Montreal.
Local transmission, however, has been detected in Toronto and other North American cities in 2023, prompting health officials to issue a warning.
Physicians must maintain their vigilance and continue to promote vaccination for people who are eligible.
— With a file from Reuters
Montreal connection behind monkeypox name change to ‘mpox’
Re-emerging levels of respiratory illness have caused increased patient numbers at the HSC Children's pediatric intensive care unit over the last week, and some non-urgent procedures may be postponed, Shared Health says.
On Thursday morning, there were 17 pediatric patients in the intensive care unit, and a considerable number of which were already experiencing health issues that were aggravated by respiratory illness. The unit's normal baseline is nine, Shared Health said in a Thursday media release.
The release said patient volumes at the children's emergency department are stable but more children with flu-like symptoms have been recorded coming in over the last two weeks, going from a low of 22 in mid-March to 47 on Wednesday.
A variety of respiratory illnesses are spreading through the community and have contributed to the increased level of patients in the pediatric intensive care unit, according to Shared Health.
Meanwhile, the number of patients in the neonatal intensive care unit was at 51 on Thursday morning, which is slightly above the unit's normal baseline capacity of 50.
Ten staff are being temporarily reassigned to the pediatric intensive care unit to deal with the increased level of patients, the release said.
Some staff are being pulled from the pediatric surgical and recovery units, which means non-urgent procedures may be postponed due to the reassignments, Shared Health said.
Families of patients impacted by the postponements will be contacted, they said, and all urgent and life-threatening surgeries will go unhindered.
Families can protect their children from respiratory illnesses by limiting their contact with people exhibiting cold-like symptoms, washing their hands frequently and staying up to date on vaccinations, Shared Health said.
Patient volumes increased last month
While overall wait times at emergency and urgent care centres were stable in February, Shared Health said daily patient volumes in the province went up.
The daily average of patients seeking care was 750 last month, which is an increase from 730.4 in January, according to a separate Thursday news release.
The average length of stay for patients in emergency or urgent care units to be transferred to an inpatient unit went down to 21.77 hours last month, which is an improvement from 22.5 hours in January, the release said.
The overall number of people who left without being seen went down last month, from 13 per cent in January to 12.1 per cent in February, according to Shared Health. It also decreased at the HSC emergency department, from 25 per cent in January to 23.4 per cent last month.
Shared Health is reminding Manitobans to continue to call 911 in case of an emergency, and said the sickest and most injured patients will remain their priority.
When Marleen Conacher was taken to a hospital for major stroke treatment for the second time in a week in 2021, she wasn't treated with a clot-busting drug like she was previously given at North Battleford Hospital in Saskatchewan.
Instead, she was transported directly to Royal University Hospital in Saskatoon, where a stroke team performed an endovascular thrombectomy (EVT).
The procedure involved passing small devices through one of the arteries in her groin, and then using suction, or tubes called stents to pull the stroke-causing blood clot out.
"I don't recall when they, they put the little claw-like thing up through my groin and it went up through the artery and, and into my brain," she said. "But I do remember feeling when they had got to it and were pulling it out."
"It was a great deal of pressure. It did not hurt, but it was a great deal of pressure," she told The Current's Matt Galloway.
Within a few days of the stroke, Conacher was out of the hospital, walking on her own and ready to go shopping.
She said she doesn't think about the stroke much these days.
"I don't spend a lot of time, you know, thinking about having a stroke or whatever or that time," she said. "I just thank the good Lord that I am here."
Marleen Conacher (centre), pictured with her two granddaughters. Physicians performed an endovascular thrombectomy on her when she suffered a stroke in July 2021. (Gray & Arbor Photography)
EVT procedures are a relatively new option in the field of ischemic stroke treatment. In 2015, a study known as the escape stroke trial led by the University of Calgary's Hotchkiss Brain Institute found that, overall, positive outcomes for stroke patients increased from 20 per cent to 55 per cent thanks to EVTs.
Today, EVTs are used in about 25 to 30 major hospitals across Canada — and according to the senior study author and stroke specialist Dr. Michael Hill, it's had a "massive treatment effect."
"People would come in and they were paralyzed on one side, they couldn't speak or they were severely affected, and they were leaving the hospital in two or three days," he told Galloway.
"That was a visible change ... whereas [before] people would have stayed many days and weeks for their recovery and rehab, if they survived at all."
Speed is critical
Hill said the key to this procedure's success is speed, as "10 or 15 minutes makes a difference."
That's why a patient is often greeted at the door by a team of emergency department nurses, physicians and the stroke specialist.
"When we're alerted to a stroke or suspected stroke syndrome and we're meeting somebody in the emergency room, we're hustling to get there and be there before the patient or just after the patient arrives," said Hill, who is a neurologist at the Foothills Medical Centre in Calgary.
WATCH: Dr. Michael Mayich explains how clots that cause strokes can be removed
New medical device removes blood clots in stroke patients in minutes
8 months ago
Duration 0:25
Dr. Michael Mayich at the London Health Sciences Centre's University Hospital explains how a new medical device from Vena Medical is used to remove clots in the brain that cause a stroke and reverse those symptoms.
From there, medical personnel conduct a clinical and imaging assessment to confirm if a patient has a blood clot and where it may be.
If the clot is in a location that is "amenable to a vascular treatment," then an EVT will be offered.
Sedation can be approached in two ways, he said.
"Sometimes, patients are completely co-operative and we can do it completely awake. Sometimes they require some degree of sedation to keep them still."
"You can imagine it's important to do this procedure with your head relatively still. You can't have them thrashing around."
Dr Michael Hill, who helped pioneer the development of thrombectomies in Canada, shows pieces of a clot retrieved from a stroke patient. (CBC)
A game-changer
Hill said EVTs have a lot of potential in improving stroke treatment, as positive outcomes are a lot more frequent.
"So it's terrific, right? We get people back to their lives," he said.
In an ideal world, of course it's available everywhere because you don't have a stroke just because you live in the middle of Calgary or the middle of Toronto, right?-Dr. Michael Hill, stroke physician
At the moment, EVTs aren't available for all Canadians. Hill said the procedure is usually reserved for patients with the most severe forms of ischemic stroke, which occurs when the blood supply to part of the brain is interrupted or reduced.
"It's a tertiary-level procedure. You're not going to see it in a small, rural hospital," he said.
But part of that has to do with the volume of cases needed in order to develop expertise in this field, and it's big hospitals in major cities that tend to see the most patients.
"So if you're just doing one a year, you're more likely to have complications than you are to be successful," he said. "Whereas if you're doing 150 a year … everyone's ready for these things to occur because you're doing it so frequently."
Still, it's important to balance that expertise with availability.
"In an ideal world, of course [EVT is] available everywhere because you don't have a stroke just because you live in the middle of Calgary or the middle of Toronto, right?" He said.
For the time being, Conacher is content with how the procedure turned out — it's been nearly two years and the only major impact the stroke has had is a bit of memory loss.
Furthermore, as someone who saw her dad suffer paralysis in his left side due to stroke, she's pleased with the way stroke treatment is evolving.
"If they had things like this, I think he would have been just as fine as I was," she said.
TORONTO — A Toronto-based neurosurgeon who has deepened our understanding of brain tumours and a northern Ontario psychologist focused on Indigenous-led mental health care are among the winners of the prestigious Canada Gairdner Awards.
The global honours, which recognize some of the world’s most significant biomedical and health research, named Dr. Gelareh Zadeh and Dr. Christopher Mushquash as the two inaugural winners of the Canada Gairdner Momentum Award.
A spokesperson for the Gairdner Foundation says the prize was introduced this year to address a gap in the awards landscape for mid-career scientists. Zadeh and Mushquash each win $50,000.
Mushquash, a psychology professor at Lakehead University and psychologist at Dilico Anishinabek Family Care, was praised for Indigenous-led mental health and substance use research that led to culturally appropriate mental health services for First Nations communities.
Reached by phone in Thunder Bay, Mushquash called the prize a "tremendous honour" and thanked the Gairdner Foundation for a chance to bring Indigenous mental health issues to the attention of a broader audience.
"When you begin to think about people as a sum of their physical and mental and emotional and spiritual selves in a broader, more holistic kind of way, it begins to open up a lot of potential for thinking about how to support people in a way that's much broader," said the 43-year-old Mushquash, who is Ojibway and a member of Pays Plat First Nation.
"This is not just important for Indigenous people. I think there's more and more awareness now within health systems in general and certainly within the public that imagining any single aspect of ourselves without the understanding of the relationship between other aspects is limiting."
Zadeh, whose many titles include professor and neurosurgery division chair at the University of Toronto, head of neurosurgery at Toronto Western Hospital and senior scientist at Princess Margaret Cancer Centre, was recognized for gains in the molecular and genomic understanding of brain tumours, leading to better ways to classify and manage brain tumour subtypes and treat patients.
Five other innovators in the fields of artificial intelligence and microbiology each nabbed the annual international award, which bestow $100,000 to each winner for influential contributions to biomedical science.
Two of the winners come from the London-based lab DeepMind, which developed an AI system that can predict the 3D shape of protein structures and was touted in the award citation for its "enormous potential to accelerate biological and medical research.”
The foundation said AlphaFold, developed by CEO and founder Demis Hassabis and senior research scientist John Jumper, has been accessed by one million researchers and users in 190 countries and been used to predict "nearly every protein known to science."
The three other winners are scientists Bonnie L. Bassler at Princeton University, E Peter Greenberg at the University of Washington and Michael R. Silverman, an emeritus investigator at The Agouron Institute.
Their collective discoveries about how bacteria communicate has spawned an entire field in microbiology that can lead to new ways to promote health and prevent disease, says their award citation.
"They have independently and collaboratively revolutionized the way we think about bacteria, completely overturning the paradigm that bacteria act independently of each other."
The John Dirks Canada Gairdner Global Health Award went to José Belizán of the Institute for Clinical Effectiveness and Health Policy Argentina for work that has improved the lives of pregnant people and their children.
The citation touted Belizán's development of low-cost global interventions during pregnancy that reduce illness and death, and promote equity in vulnerable populations.
The Gairdner Awards are nicknamed the "baby Nobels" because organizers say 96 Gairdner winners have gone on to receive Nobel Prizes.
A virtual event was set to celebrate the winners Thursday morning.
The laureates will formally receive their medal at a gala in Toronto on Oct. 26.
This report by The Canadian Press was first published March 30, 2023.
COVID, cold and flu clinics (CCFCC) in Brantford, Brant and Norfolk will permanently close on Friday, March 31.
Article content
“After this date, if patients require a COVID-19 test, viral symptom assessment, or treatment, there are many local options available to them,” said Jessica Ackland, communications coordinator for the Brantford Brant Norfolk Ontario Health Team.
Introduced as clinical assessment centres early in the pandemic, the CCFCCs provided testing swabs, primary care assessment and management of patients who exhibited symptoms of the virus.
The clinics also served as an alternative to emergency departments and urgent care centres at the height of the pandemic.
Initially at the Brantford Convention Centre before relocating to the Willett Urgent Care Centre in Paris, the Brantford Brant CCFCC saw 140,861 patients since the spring of 2020.
Article content
The Norfolk CCFCC at the Delhi Community Centre with support from the Norfolk Family Health Team saw 2,607 patients since opening in September 2022.
Anyone seeking a COVID-19 test, assessment or treatment after March 31, 2023, can contact their family doctor or nurse practitioner or locate a pharmacy that provides testing.
The public can also call 811 or visit ontariohealth.ca/health811 for information about testing, assessment, and treatment.
To find an open assessment centre visit Ontario.ca/assessment-centre-locations.
Patients who think they may have COVID-19 should not delay in seeking treatment that should begin within five days of symptom onset.
Adults with severe symptoms that include shortness of breath, confusion, chest pain, and loss of consciousness, and children that exhibit difficulty breathing, bluish skin, or are unable to drink or breastfeed are urged to call 911 or go to the nearest emergency department.
WEDNESDAY, March 29, 2023 (HealthDay News) -- New advice from the World Health Organization (WHO) says healthy children and teens may not need additional COVID-19 shots, though they may need to catch up on other routine vaccines.
“The public health impact of vaccinating healthy children and adolescents is comparatively much lower than the established benefits of traditional essential vaccines for children – such as the rotavirus, measles and pneumococcal conjugate vaccines,” the WHO’s Strategic Advisory Group of Experts on Immunization (SAGE) said Tuesday in a news release.
Instead, COVID-19 vaccines should go to high-risk people.
"Updated to reflect that much of the population is either vaccinated or previously infected with COVID-19, or both, the revised roadmap reemphasizes the importance of vaccinating those still at-risk of severe disease,” said SAGE chair Dr. Hanna Nohynek.
People are also reading…
So, SAGE now recommends additional booster doses for older people, immunocompromised people of all ages, front-line health workers and pregnant people six or 12 months after their last booster dose. Those are included in the high-priority group.
In the middle are children and adolescents who have health risks, as well as healthy adults younger than 60. SAGE now recommends they receive primary vaccines and first boosters. It does not recommend additional boosters.
Countries should consider disease burden and cost-effectiveness when deciding whether to vaccinate healthy kids aged 6 months to 17 years old.
Nohynek noted the need to vaccinate children for other diseases, including measles. Cases for that vaccine-preventable disease are rising around the world, CNN reported.
Polio, too, is spreading in several areas. WHO vaccine advisors recommend improving vaccine coverage, CNN reported, as well as using a dose of injectable polio vaccine when there is “persistent poliovirus circulation.”
“As we all know, the COVID pandemic has taken a heavy toll on immunization programs,” Nohynek said. “It’s been a tremendous effort, and many countries have done very well reaching high coverages, but it is still requiring efforts to reduce the inequities, and we need to reach the high-priority groups, and we need to close the coverage gaps.”
More information
The U.S. Centers for Disease Control and Prevention has COVID-19 vaccine guidance.
The U.S. Food and Drug Administration on Wednesday approved selling the leading version of naloxone without a prescription, setting the overdose-reversing drug on course to become the first opioid treatment drug to be sold over the counter.
It’s a move that some advocates have long sought as a way to improve access to a life-saving drug, though the exact impact will not be clear immediately.
Here’s a look at the issues involved.
WHAT IS NARCAN?
The approved nasal spray from Gaithersburg, Maryland-based Emergent BioSolutions is the best-known form of naloxone.
It can reverse overdoses of opioids, including street drugs such as heroin and fentanyl and prescription versions including oxycodone.
Making naloxone available more widely is seen as a key strategy to control the nationwide overdose crisis, which has been linked to more than 100,000 U.S. deaths a year. The majority of those deaths are tied to opioids, primarily potent synthetic versions such as fentanyl that can take multiple doses of naloxone to reverse.
The drug has been distributed to police and other first responders nationwide.
Advocates believe it's important to get naloxone to the people who are most likely to be around overdoses, including people who use drugs and their relatives.
The decision "represents a decisive, practical and humane approach to help people and flatten the curve of overdose deaths,” said Chuck Ingoglia of the National Council for Mental Wellbeing, in a statement.
___
WHAT DOES THE FDA APPROVAL MEAN?
Narcan will become available over-the-counter by late summer, the company said.
Other brands of naloxone and injectable forms will not yet be available over the counter, but they could be soon.
Several manufacturers of generic naloxone that's made similarly to Narcan will now be required to file applications to switch their drugs over the counter as part of a requirement by the FDA.
The nonprofit Harm Reduction Therapeutics Inc., which has funding from OxyContin maker Purdue Pharma, already has an application before the FDA to distribute its version of spray naloxone without a prescription.
___
HOW IS NALOXONE DISTRIBUTED NOW?
Even before the FDA's action, pharmacies could sell naloxone without a prescription because officials in every state have allowed it.
But not every pharmacy carries it. And buyers have to pay for the medication — either with an insurance co-pay or for the full retail price. The cost varies, but two doses of Narcan often go for around $50.
The drug is also distributed by community organizations that serve people who use drugs, though it's not easily accessible to everyone who needs it.
Emergent has not announced its price and it's not clear yet whether insurers will continue to cover it as a prescription drug if it's available over the counter.
FDA Commissioner Robert Califf in a statement encouraged Emergent to make the drug available “at an affordable price."
___
DOES MAKING NALOXONE OVER-THE-COUNTER IMPROVE ACCESS?
It clears the way for Narcan to be made available in places without pharmacies — convenience stores, supermarkets and online retailers, for instance.
Jose Benitez, the lead executive officer at Prevention Point Philadelphia, an organization that tries to reduce risk for people who use drugs with services including handing out free naloxone, said it could help a lot for people who don't seek services — or who live in places where they're not available.
Now, he said, some people are concerned about getting naloxone at pharmacies because their insurers will know they're getting it.
“Putting it out on the shelves is going to allow people just to pick it up, not have stigma attached to it,” he said.
But it remains to be seen how many stores will carry it and what the prices will be. The U.S. Centers for Medicare and Medicaid Services, which now cover prescription naloxone for people on the government insurance programs, says that coverage of over-the-counter naloxone would depend on the insurance program. The centers have not given any official guidance.
Maya Doe-Simkins, a co-director of Remedy Alliance/For The People, which launched last year to provide low-cost — and sometimes free — naloxone to community organizations, said her group will continue to distribute injectable naloxone.
___
ARE THERE DRAWBACKS TO OVER-THE-COUNTER SALES?
One concern is whether people who buy Narcan over-the-counter will know how to use it properly, said Keith Humphreys, a Stanford University addiction expert, though the manufacturer is responsible for clear directions and online videos on that.
One benefit of having pharmacists involved, he said, is that they can show buyers how to use it. One key thing people need to be reminded of: Call an ambulance for the person receiving naloxone after it's been administered.
He also said there are fears that if the drug isn't profitable as an over-the-counter option, the drugmaker could stop producing it.
___
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Science and Educational Media Group. The AP is solely responsible for all content.
A newly released survey finds nearly all Canadian adults had antibodies against COVID-19 for about half of 2022, with most acquiring them through a previous infection.
The results, released Tuesday by Statistics Canada in partnership with the Public Health Agency of Canada and COVID-19 Immunity Task Force, show that 98.1 per cent of Canadian adults living in the country's 10 provinces had antibodies against SARS-CoV-2, the virus that causes COVID-19, between April and August 2022.
These individuals acquired antibodies through either vaccination, previous infection or both.
Over that five-month period, 53.9 per cent developed antibodies through a past infection.
This is in comparison to the results of a previous version of the survey done between November 2020 and April 2021 that found 2.6 per cent of Canadians had COVID-19 antibodies due to a previous infection.
A report detailing the findings says while almost 54 per cent of Canadians surveyed had antibodies from an infection, the actual proportion of those infected since the start of the pandemic is likely higher.
"This is due, in part, to the fact that an antibody response to an infection may not always be detectable, especially among those who are vaccinated who may generate fewer antibodies following a subsequent infection. In addition, antibody levels can decrease over time," the report says.
ANTIBODIES
The survey used a technique known as dried blood spot testing to detect COVID-19 antibodies from vaccination or a past infection, as well as saliva samples to determine a current or recent infection.
A total of 105,998 people were chosen to participate in the survey, of which 30.7 per cent completed a questionnaire asking about general health and exposure to COVID-19. Of those who completed the questionnaire, nearly 54 per cent provided a blood sample and 54.5 per cent provided a saliva sample.
The body produces antibodies to defend against diseases and in response to vaccination.
However, they do decrease over time and the report says some people previously infected with COVID-19 or who have been vaccinated may no longer have detectable levels of antibodies.
But while antibodies may decrease with time, the report says it does not mean a person's immunity has waned.
Rather, an individual may have developed cell-mediated immunity, which activates specialized white-blood cells called T cells.
The report says dried blood spot testing also does not measure cell-mediated immunity.
Even without detectable antibodies, the report adds that cell-mediated immunity could be enough to protect someone against severe COVID-19 symptoms. The mere presence of antibodies alone also isn't enough to suggest a person could fend off a new infection or any serious symptoms.
MANY UNAWARE THEY WERE INFECTED
The survey found as many as two out of five Canadians with antibodies from a previous infection were unaware they had been infected, either because they never tested positive or did not suspect an infection.
Among those who previously tested positive for COVID-19, antibody levels were higher between 14 and 90 days post-infection before gradually decreasing over time.
"While this is indicative of decreasing antibodies, there are other factors which could impact this analysis," the report says.
"For example, since vaccines may lead to a lesser antibody response following an infection, the percentage of Canadians with antibodies from infection may be affected by changing vaccination rates over time. Further, since the survey focuses on first infections, re-infections would also impact this analysis as these could lead to a rebound in antibody levels."
Canadians with a disability or underlying health conditions were less likely to have antibodies from a previous infection compared to those who did not report a disability or health condition.
Those 18-34 and 35-49 were also more likely to have antibodies from a previous infection than older Canadians were.
Antibody levels from infection varied between population groups, ranging from as low as 53 per cent for Chinese Canadians to as high as 80.7 per cent for Black Canadians.
Across provinces, Nova Scotia had the lowest proportion of residents who developed antibodies from infection at 46.5 per cent, while Quebec (56.5 per cent), Alberta (57.4 per cent) and Saskatchewan (57.4 per cent) had the highest rates.
The survey did not include data from the three territories, those under 18 or people living on reserve, in institutions or Canadian Forces Bases.
(Bloomberg) -- Healthy children and adolescents may no longer need Covid shots, the World Health Organization said, updating its guidance on vaccines as the world adjusts to living permanently with the virus.
Older people and higher-risk groups — including those with underlying conditions — should get Covid boosters between six and 12 months after their last injections, the WHO said in a statement announcing a revised vaccine road map for the new stage of the pandemic.
“Countries should consider their specific context in deciding whether to continue vaccinating low-risk groups, like healthy children and adolescents, while not compromising the routine vaccines that are so crucial for the health and well-being of this age group,” said Hanna Nohynek, chair of the WHO’s Strategic Advisory Group of Experts on Immunization.
The Geneva-based organization’s latest advice comes as booster rates fall in countries from China to the US, with just 16% of Americans lining up for the latest round of shots targeting the omicron variant, Bloomberg reported earlier this month.
The dropoff won’t just have financial consequences for vaccine makers — including Pfizer Inc. and Moderna Inc. — but is also sparking concerns among public health experts who say updated vaccinations are the best way to protect against Covid.
Read more: Covid Boosters Sour for Pfizer, Moderna With Uptake Rate at 16%
Healthy children between the ages of 6 months and 17 years are a low-priority group for vaccination, the WHO said, and primary and booster doses are safe and effective for them. They have typically experienced less severe reactions to Covid than adults.
The WHO said context mattered in deciding whether to inoculate younger people given the lower burden of disease.
The organization “urges countries considering vaccination of this age group to base their decisions on contextual factors, such as the disease burden, cost effectiveness, and other health or programmatic priorities and opportunity costs,” the statement said.
The World Health Organization on Tuesday changed its recommendations for COVID-19 vaccines, suggesting that high-risk populations should receive an additional dose 12 months after their last booster.
The health agency defined high-risk populations as older adults, as well as younger people with other significant risk factors. For this group, the agency recommends an additional shot of the vaccine either 6 or 12 months after the latest dose, based on factors such as age and immunocompromising conditions.
The WHO defined the group including healthy children and adolescents as “low priority” and urged countries to consider factors like disease burden before recommending vaccination of this group.
The recommendations come as countries take differing approaches for their populations. Some high-income countries like the United Kingdom and Canada are already offering high-risk people COVID-19 boosters this spring, six months after their last dose.
The WHO said this was an option for a subset of people who were at particular risk, but its recommendations were intended as a best practice global guide.
Earlier this month, the National Advisory Committee on Immunization (NACI), advised Canadians at risk of severe illness due to COVID get an additional booster dose this spring.
COVID-19 apathy: vaccination rates slowing three years into pandemic
NACI said that includes adults 80 and up, those living in long-term care homes and other congregate settings for seniors or those with complex medical needs.
It also advised adults 18 and older who are moderately to severely immunocompromised, either due to medical treatment or an underlying health condition, to get a booster shot.
The agency said its committee of experts had also said that additional booster vaccines for COVID beyond the initial series – two shots and a booster – were no longer routinely recommended for “medium risk” people.
With files from the Canadian Press
(Reporting by Bhanvi Satija in Bengaluru and Jennifer Rigby in London; Editing by Shailesh Kuber)
Assistant Professor of Kinesiology Stephen Klassen researches how the brain ‘talks’ to a large network of blood vessels that regulate blood pressure and blood flow in humans.
Stephen Klassen is a communications specialist, but not in the usual sense of the term. He studies the language of the brain, specifically how the brain ‘talks’ to a large network of blood vessels that regulate blood pressure and blood flow in humans.
To do so, the Assistant Professor of Kinesiology uses a method called microneurography, which visualizes and records nerve impulses travelling from the brain and brainstem towards blood vessels in humans.
Baroreceptors in the arteries sense when blood pressure falls. They relay this information to the brain, which changes the neural signals towards the blood vessels and the heart.
Reacting to these signals, the blood vessels then constrict and the heart beats faster and harder, which ensures that blood pressure remains optimal. The opposite process occurs when blood pressure rises too high.
The neural messages Klassen’s lab studies are those of the sympathetic nervous system, known best for its ‘flight-or-fight’ role that elevates heart rate and regulates blood flow for oxygen delivery to help the body cope with dangerous or stressful situations.
Related to that is the parasympathetic nervous system, a process in which the brain and nerves communicate with the heart to slow heart rate and decrease blood pressure during times of relaxation.
Assistant Professor of Kinesiology Stephen Klassen (left) performs an ultrasound of the blood vessels in the neck of PhD student Nathan Iannarelli (laying on bed). Klassen and his team research the brain circulatory connection.
The new insight in Klassen’s latest baroreflex paper, pre-published March 22 in the Journal of Neurophysiology, comes from closely examining the role of ‘action potentials’ in the baroreceptor reflex.
An action potential is a rapid rise and subsequent fall of electrical currents in the membranes of neuron and muscle cells. This process means the neuron is ‘firing’ and ‘communicating.’
“Action potentials are the most basic strategy used by our neurons to ‘communicate’,” says Klassen. “Previously, studies had not looked this deeply into the neural messages directed towards the blood vessels in the context of baroreflex regulation during exercise.”
Due to the activity of action potentials, Klassen and his team found that the baroreceptor reflex strongly controls only some, but not all, sympathetic neurons communicating with blood vessels during exercise in humans.
“We will continue our exploration to understand the unknown pathways that control other sympathetic neurons during exercise,” says Klassen.
The research team also found that the strength of baroreflex control over human sympathetic neurons can be changed during exercise.
“When muscle becomes fatigued during exercise, it sends signals to the brain that increase baroreflex control of some of our sympathetic neurons controlling blood vessels,” says Klassen.
“On the other hand, areas in our brain that control how much effort we are putting in during exercise might reduce the baroreflex control of sympathetic neurons communicating with blood vessels,” he says.
This latest research adds to the ways Klassen is expanding research in his field. For instance, in another study, Klassen and his team used a new approach to record participants’ nerve activity and found that previous studies may have been underestimating the amount of sympathetic neural signals towards human blood vessels by about 30 percent, in young healthy participants.
“This previous study provided us with a more complete picture of the language that the brain uses to communicate with our blood vessels to control our blood pressure and keep us alive,” says Klassen.
Klassen, who is a research collaborator at Mayo Clinic in Minnesota, conducts what is known as ‘fundamental research.’ This type of research develops a greater understanding of how natural processes work or improving scientific theories.
Last year, he received a grant from the Natural Sciences and Engineering Research Council of Canada (NSERC) to examine the mechanisms the sympathetic nervous system uses to control the cardiovascular system.
“My NSERC-funded research will improve our basic physiological understanding of neurocirculatory regulation,” says Klassen.
“Also, this research has implications for better understanding the development of cardiovascular risk factors and cardiovascular diseases such as hypertension and coronary artery disease, as the sympathetic nervous system plays a critical role in their development,” he says.
Klassen is scheduled to present the results of his ongoing research at the American Physiological Society Conference in Long Beach, California in April this year.