Peel Region has its first confirmed case of monkeypox.
According to Peel Public Health, the person infected is an adult male in his 30s who lives in Mississauga.
The heath unit said the risk to the public remains low.
Monkeypox, which comes from the same virus family as smallpox, spreads though close contact with an infected individual. Most transmission happens through close contact with the skin lesions of monkeypox, but the virus can also be spread by large droplets or by sharing contaminated items.
To reduce risk of infection, people are advised to be cautious when engaging in intimate activities with others. Vaccination is available for high-risk contacts of cases and for those deemed at high risk of exposure to monkeypox.
Symptoms can include fever, headache, fatigue, swollen lymph nodes, and a rash/lesions, which could appear on the face or genitals and then spread to other areas.
Anyone who develops these symptoms should contact their healthcare provider and avoid close contact with others until they have improved and rash/lesions have healed.
While most people recover on their own without treatment, those who have been in close contact with someone who has tested positive for monkeypox should self-monitor for symptoms, and contact PPH to see if they are eligible for vaccination.
The Mississauga case is at least the 34th confirmed case of the disease in Ontario, with dozens more under investigation.
Cat and dog owners who cuddle their pets when infected with COVID-19 could end up making the animals sick with the virus, according to a Canadian study.
The study said that while it was already known that animals including cats, dogs, ferrets and hamsters seem to be susceptible to COVID-19, transmission may be happening more often than previously thought.
The research, published this month in the journal Emerging Infectious Diseases, involved 69 cats and 49 dogs, including pets and animals from shelters and neuter clinics.
Pet owners were also asked to fill out an online survey about the nature of their interaction with their animals.
“These data indicate relatively common transmission of SARS-CoV-2 from humans to animals and that certain human-animal contacts — example, kissing the pet, pet sleeping on the bed — appear to increase the risk,” said the study.
“We inferred that infections in dogs and cats reflect direct transmission from humans to animals, given the pandemic nature of this virus in humans and limited contact of most household pets with other animals.”
Dogs and cats that lived in shelters showed lower rates of COVID-19 infection compared with those that lived with humans, said study co-author Prof. Scott Weese of the University of Guelph’s Ontario Veterinary College.
“It was a fairly substantial difference as we would have expected,” said Weese.
Lead author Prof. Dorothee Bienzle from the University of Guelph’s pathobiology department said results suggest that cats have a higher rate of COVID-19 infection than dogs.
“It has to do with how well the virus latches on to the receptor in the cat or dog’s respiratory system,” said Bienzle.
The high prevalence of COVID-19 antibodies in cats surprised researchers, she said.
“We did not expect quite that many,” she said. “Over half of the cats that live in a household of a person who had COVID had antibodies. That’s very high.”
Animals infected with COVID-19 show symptoms similar to humans who fall sick with the virus, she said.
“They don’t have any appetite, they feel crummy, they sleep more, they might sneeze and cough,” she said.
Weese said cats are able to pass on the infection to each other, and also to humans.
A veterinarian in Thailand was diagnosed with COVID-19 in August 2021, after being sneezed on by an infected cat owned by a patient who had tested positive for the virus, he said. Genetic analysis showed that the virus was transmitted from the cat owner to the pet and onto the veterinarian, Weese said.
There is also evidence that minks infected by humans can pass the virus on to other people, he said.
Transmission from humans to animals can be minimized by owners keeping their distance, wearing a mask and taking other precautions, just as they would to prevent infecting a person, he said.
“Ideally, what we want to do is keep it from spreading as much as possible so people can limit the contact they have with animals when they’re infected,” he said. “That’s ideal.”
This report by The Canadian Press was first published June 26, 2022.
A 32-year-old woman with a history of an early pregnancy loss followed by a term birth presented to her gynecologist with difficulty conceiving and amenorrhea. Her second pregnancy, the live birth, had resulted in a vaginal delivery followed by manual removal of an adherent posterior placenta. Twenty months postpartum, she had ongoing amenorrhea, despite not breastfeeding. Endocrine investigations for follicle-stimulating hormone, luteinizing hormone, thyroid-stimulating hormone and prolactin were normal.
We ordered transvaginal ultrasonography, which showed a hyperechoic endometrial stripe (Figure 1). We performed a hysteroscopy and resected bony spicules overlying the posterior wall and uterotubal regions (Figure 2). The pathology examination showed multifocal calcific deposits and metaplasia, with a background atrophic endometrium. We diagnosed osseous metaplasia with secondary infertility. Her menses subsequently resumed; she spontaneously conceived and had a healthy live birth.
The prevalence of osseous metaplasia is estimated to be about 0.02% among women with infertility.1 More than 80% of reported cases occur after a pregnancy.2 Osseous metaplasia causes a sterile foreign body reaction similar to that caused by an intrauterine contraceptive device (IUCD). Risk factors include previous uterine instrumentation, the presence of an IUCD, infection, uterine anomalies and retained products of conception.3 Clinicians should consider osseous metaplasia when sonograms show echogenic bands with acoustic shadowing. Hysteroscopy is recommended, with resection of calcifications often re-establishing menses and fertility.2,3
Several pathophysiological explanations have been suggested for the development of osseous metaplasia. Multipotent stromal cells may occur as a response to chronic endometritis, an emerging risk factor for recurrent pregnancy loss and implantation failure. In addition, osseous differentiation from mesenchymal stem cells may occur secondary to osteogenesis after retention of fetal bones, dystrophic calcification of retained necrotic tissues and disorders of calcium and vitamin D metabolism.3.
Clinical images are chosen because they are particularly intriguing, classic or dramatic. Submissions of clear, appropriately labelled high-resolution images must be accompanied by a figure caption. A brief explanation (300 words maximum) of the educational importance of the images with minimal references is required. The patient’s written consent for publication must be obtained before submission.
Two pet rabbits have died after becoming infected with a highly contagious virus that has been newly detected in Ontario, sparking concern among vets and pet owners.
The rabbits were from the same household and were previously healthy, according to Dr. Jamie McGill Worsley, a vet in Forest, Ont., in Lambton County.
The rabbits quickly passed away.
"This was devastating for a pet owner with no warning and initially no understanding," she said, "As we did testing, we started to become more suspicious that maybe this [virus] was the case."
Samples were sent to a lab, and earlier this month the Canadian Food Inspection Agency confirmed it was rabbit hemorrhagic disease virus (RHDV-2).
The Canadian Food Inspection Agency (CFIA) said it was the first time that RHDV-2 has been detected in the province, though it has previously been found in B.C. and Alberta.
The source of the infection isn't known, the agency said.
"Immediately following this, the CFIA placed a quarantine on the site," the agency said in a statement. "An investigation has been completed and no high risk contacts have been identified that could result in spread of the disease from this premise. The CFIA is collaborating with the province and continues to monitor the situation."
What is RHDV-2
According to the CFIA, the disease is highly contagious in wild and domestic rabbits. The virus doesn't affect other species.
People can pick up the virus on their shoes — or even on their vehicle's tires — through the feces of an infected rabbit, said McGill Worsley.
That's one of the reasons why the virus is of such great concern, she said.
"It is very resilient in the environment. It's very easy to spread around with microscopic amounts. And then, of course, the potential outcome of this virus, its impact on the rabbits, whether they're wild or pet rabbits, is quite devastating," said McGill Worsley, who has strengthened disinfection protocols at her clinic because of the virus.
Dr. Jamie McGill Worsley of Forest Veterinary Clinic in Forest, Ont., is shown with a pet rabbit at her clinic. (Submitted by Jamie McGill Worsley )
The CFIA said that infected rabbits usually show symptoms within one to five days. Symptoms include fever, loss of appetite and neurological symptoms such as difficulty walking.
"Death is common after a short period of illness. Death may also occur suddenly without signs," the CFIA said in a fact sheet on its website.
Rabbit owner Hazel Gabe of Ottawa is part of a Facebook group for rabbit owners where news of the virus has generated concern.
"People are really scared. People are very scared and nervous," she said.
But for some, there's a little bit of relief, she said.
"Now that there's been some cases in Ontario, even though we hate that some rabbits died and somebody probably lost their pet. But this means that maybe we will finally have access to the vaccine, because we've been asking for this for a while."
While other countries have vaccines that protect rabbits against the virus, there's not one readily available in Canada.
Hazel Gabe, shown with her pet rabbit, wants to see a vaccine against rabbit hemorrhagic disease virus become more widely available. (Sonya Varma/CBC)
In B.C., where there have been outbreaks, the government waited until there were a certain number of cases before offering an organized vaccine program.
McGill Worsley suspects the case will be the same in Ontario. But at this point, clinics have to request a special permit to import the vaccine from Spain or France, she said.
"It's a bit of a process. I've worked part way through it myself ... that way we can start to be able to protect rabbits once we have permission from the Canadian Food Inspection Agency to bring those vaccines here."
Former senior civil servant and diplomat Norman Spector shared a fascinating article with me this weekend from the Ottawa Citizen.
A family physician in the national capital, Dr. Nili Kaplan-Myrth, hoped to conduct mass vaccinations for people who want a fourth dose of COVID-19 but don't qualify under Ontario's rules.
She reportedly wanted to create a large outdoor "jabalooza" clinic but health officials refused to provide her with vaccines.
Ontario restricts access to fourth shots of COVID-19 vaccines to those who are 60 years of age or older.
Next door in Quebec, people can get fourth shots if they are 18 and older.
"I am receiving lots of individual requests for help," Kaplan-Myrth tweeted on Sunday (June 26). "I can't give you the vaccine at this time, but hands up (and DM) if you as plaintiffs want to bring this to court as a group. Would require a litigation team."
There's a tremendous amount of scientific data showing that COVID-19 vaccines lessen the severity of COVID-19. They reduce the likelihood of dying or being hospitalized from the disease.
However, COVID-19 vaccine effectiveness wanes over time. This is why Kaplan-Myrth is such a strong advocate for booster shots. She believes that these boosters are particularly important when so many people are not wearing masks indoors.
Keep in mind that COVID-19 initially presents as a respiratory infection.
In some cases, however, it causes serious brain injuries and cardiovascular problems. It's especially dangerous for the immunocompromised, who are at higher risk of suffering severe COVID-19.
In B.C., you have to be 70 years of age or older and have gone six months since a previous COVID-19 vaccination to qualify for a fourth dose.
There are exceptions: Indigenous people, for example, can get a fourth dose if they're 55 or older.
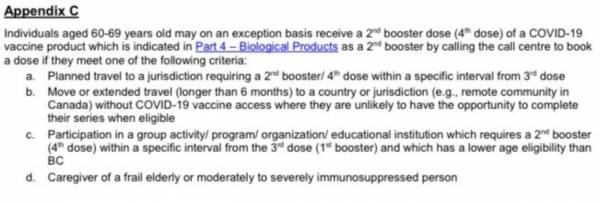
Below, you can read other exceptions listed by the B.C. Centre for Disease Control for those between the ages of 60 and 69.
The B.C. Centre for Disease Control listed these exemptions, which qualify someone from 60 to 69 years old for a fourth COVID-19 vaccination.
However, when the Georgia Straight asked the Ministry of Health about who qualified for a fourth COVID-19 vaccination, it did not include what's written after the letter "d": "Caregiver of a frail elderly or moderately to severely immunosuppressed person".
So it remains unclear in B.C. if a person between 60 and 69 who is a caregiver for either a frail elderly person or a moderately to severely immunosuppressed person is able to receive a fourth COVID-19 vaccination.
Yet it seems pretty clear from the exemptions above that if you are a cancer survivor or have kidney disease or have heart disease or have multiple sclerosis or have had a transplant and you're under 70 in B.C., you will not qualify for a fourth COVID-19 vaccination under existing rules.
Why is B.C. being more restrictive with COVID-19 booster shots than Ontario, Quebec, Saskatchewan (where you only need to be 50-plus), as well as the entire United States?
Health Minister Adrian Dix needs to come clean on that.
What possible justification is there for withholding a fourth COVID-19 shot for British Columbians under 70, especially the immune-compromised, when 226,000 vaccine doses are set to expire next month?
Why is Dix so convinced that he knows better than the governments of Ontario, Quebec, and Saskatchewan?
Some on social media are speculating that the booster shots are being withheld as part of a population-level experiment—conducted without the people's consent—on the efficacy of delaying second booster shots.
Dix and provincial health officer Dr. Bonnie Henry, through their actions, are giving oxygen to this hypothesis.
Who knows? There might even be a scientific justification for withholding booster shots.
But in the absence of evidence provided by the B.C. government, the health minister must get in front of a microphone on Monday (June 27) and provide a coherent explanation.
Failure to do so will only fuel more suspicion about the motives behind the government's policy.
Perhaps it's worth noting that in January 2021, Sciencepublished a study involving 188 people, which offered a glimmer of hope.
It showed that more than 95 percent of those who had recovered from COVID-19 had immune systems demonstrating "durable" memories of the virus, lasting up to eight months.
This prompted speculation on the National Institutes of Health website that the immune systems of those who are vaccinated would have lasting memories of the virus.
But a study of 188 people is insufficient as the basis for an entire provincewide policy.
Some might wonder if the government isn't making fourth doses of COVID-19 vaccines available to those under 70 because of the cost of distribution or due to the labour shortage in the health-care sector.
Others might suspect it's because the B.C. government thinks everyone is going to get COVID-19 anyway, so why bother?
If that's the real reason, it's a monumental disservice to those with compromised immunity. This should demand a response from Human Rights Commissioner Kasari Govender that goes well beyond writing a letter to Henry. Like by holding a public inquiry under section 47.15 of the B.C. Human Rights Code.
In the meantime, show us the evidence, Minister Dix, for why so many British Columbians are being denied a fourth COVID-19 vaccination.
And if you're unwilling to do that, then please step aside so another health minister can do this in your place.
More than 455,000 people in the Kingston region have been vaccinated against COVID-19.
Now health officials say they’re using the summer months, with low infection rates, to look ahead to what fall might bring, urging those who are still eligible to get vaccinated do so.
“Large, mass immunization clinics, mobile clinics, drive-thru clinics and small primary care clinics doing their own vaccine,” said Brian Larkin with KFL&A Public Health.
Infectious disease expert Dr. Gerald Evans says those who are still eligible for a third and fourth dose should take advantage and roll up their sleeves during the low-infection summer months.
“Now in 2022, although you still might get COVID, you’re probably not going to be very sick. You are less likely to transmit and ultimately that’s one of the ways we’re going to control the pandemic,” added Evans.
He expects another wave of COVID-19 to hit in late October to early November and that a booster may be made available for those younger than 60 who still aren’t eligible for a fourth dose.
“The best case scenario is a few more years of watching rises in cases, getting boosters to control things and ultimately getting out of it with this being just another coronavirus that just tends to cause a respiratory infection and worst-case scenario is a new variant where all the potential possibilities exist to have a big surge in cases and hopefully not a lot more serious illness,” said Evans.
Public Health says they’re still waiting for direction from the province on what’s to come this fall.
“We’re expecting that we would see more age groups and younger age groups be eligible for more doses or boosters but about when those ages start, we have yet to have that confirmed,” said Larkin.
The last 18 months of vaccines paving the way for the new normal could mean a yearly COVID booster alongside the annual flu shot.
Latest data suggests rich countries are likely to have already secured majority of next generation COVID vaccines
Less than half (49 per cent) of the 2.1 billion COVID vaccine donations promised to poorer countries by G7 countries have been delivered, according to new figures published today by Oxfam and the People’s Vaccine Alliance.
On the eve of this year’s G7 Summit, taking place in the German Alps, a new analysis shows that had the missing donated doses been shared in 2021,it could have been enough to save almost 600,000 lives in low and middle income countries, the equivalent of one every minute.
The worst offenders are the UK and Canada, who have failed to deliver anywhere near the number of vaccines they promised. Just 39 per cent of the100 million doses the UK pledged to deliver by the end of this month have actually been delivered. While the deadline to meet their respective commitments isn’t until the end of the year, only 30 per cent of Canada’s 50.7 million doses and 46 per cent of the 1.2 billion pledged by the US have been delivered. So-called ‘Team Europe’ have collectively delivered just 56 per cent of the 700 million doses promised by the middle of 2022 and Japan has delivered 64 per cent of the 60 million doses it said it would send.
Latest data from Airfinity suggests that rich nations may have already secured over half (55 per cent) of the new generation of Omicron-specific mRNA COVID-19 vaccines being developed by Moderna and Pfizer/ BioNTech. This is even before they have been approved for use, making it likely that many developing countries will yet again be left at the back of the queue.
Max Lawson, Head of Inequality Policy at Oxfam and Co-Chair of the People’s Vaccine Alliance, said: “On every level, rich nations have massively betrayed poor countries when it comes to COVID vaccines. First, they stockpiled all the supply for themselves, then they promised to donate their leftovers, but hundreds of millions of these doses never materialised.
“Rich nations are already hoarding the new generation of Omicron specific vaccines, whilst people in poorer countries will be forced to continue to face new variants with vaccines that are increasingly ineffective. The only way to fix this is to give nations the rights to make their own, not rely on rich countries to pass on doses they no longer need and deliver too late for the millions who have died.”
New data published yesterday by Imperial College London found that 599,300 deaths could have been averted in 2021 had 40 per cent of people in all countries been fully vaccinated. The billion missing doses that G7 countries failed to deliver would have been enough to reach this target. Nearly all these preventable deaths were in low- and middle-income countries.
To date only 14 per cent of people in low-income countries and 18 per cent of people on the African continent are fully vaccinated – far from the target to have 70 per cent coverage in all nations by the middle of the year. Despite such low vaccine coverage, the Imperial College research found COVID vaccines have saved 446,400 lives in Africa and 180,300 in low-income countries
At the same time, rich nations led by the EU and UK have forced through a text at the WTO which has failed to waive intellectual property on vaccines, treatments and technology that would have enabled developing countries to produce their own generic vaccines. Instead, the text adds even more bureaucratic hurdles and further protects the hugely profitable monopolies of firms such as Pfizer/BioNTech and Moderna. The People’s Vaccine Alliance is calling on all countries facing shortages of vaccines, tests and treatments to save lives and end the pandemic by using all trade rule flexibilities available and circumventing WTO rules if necessary. They say the G7 and other rich countries must not stand in their way.
The campaign groups also says that the model of leaving developing countries to rely on donations in order to vaccinate people is completely flawed and actually leads to frustration and mistrust.
Julia Kosgei, Policy Advisor at The People’s Vaccine Alliance said: “Hundreds of thousands of lives have been saved in Africa by the vaccines, but so many more deaths could have been prevented. Vaccination programs have worked best when doses have arrived on time, allowing governments to plan and scale up distribution. But many countries waited a year to get their first doses. When doses finally arrived, they came all at once, often close to their expiry date, which is totally unmanageable and unfair for countries that have already struggling health systems.
“Developing countries do not want to have to wait for leftovers, they want the reliability and dignity of being able to produce their own doses. It is a disgrace that rich countries stalled negotiations on an IP waiver to scale up vaccine production across the world so that pharmaceutical corporations could maximise profits while people died without access. To add insult to injury they couldn't even be bothered to ensure timely access to the doses they didn't even need.
“Rich countries have demonstrated that they cannot be trusted to act in the interests of public health for everyone, everywhere - it's time for leaders from the global south to take matters into their own hands. We hope that governments will do whatever is needed to protect their populations – whether that is using flexibilities in global intellectual property rules or circumventing them to save lives. Rich countries must not get in their way.”
Previous research by the People’s Vaccine Alliance found that vaccine monopolies are making it 5 times more expensive to vaccinate the world, while Moderna and Pfizer / BioNTech are making over $1,000 profit every second from COVID vaccines.
/Ends
For more information, or to arrange an interview please contact the Oxfam Press office on: +44 (0)7748 761999 media.unit@oxfam.org.uk
Notes to editors:
On Saturday 25 June an Oxfam ‘Big Heads’ photo opportunity will be taking place from 10.30am local time in Munich. Campaigners dressed as G7 leaders in hiking outfits will have to choose the right path to fight the COVID pandemic, standing at a big signpost with two directions, towards “Corporate profits” or “Saving lives”. For more information, please see the Media Advisory: https://oxfam.app.box.com/s/eg10zdy3w7x7rwbwwnouvx50ey2u4klz